Part 10 established that regulatory models constrain what counts as “proof.”
Now we go one layer deeper and examine how funding, institutional alignment, and economic incentives influence which research questions get prioritised, amplified, or normalised.
The focus is structural influence — not conspiracy, not intent — but incentive architecture.
Science Operates Within Systems
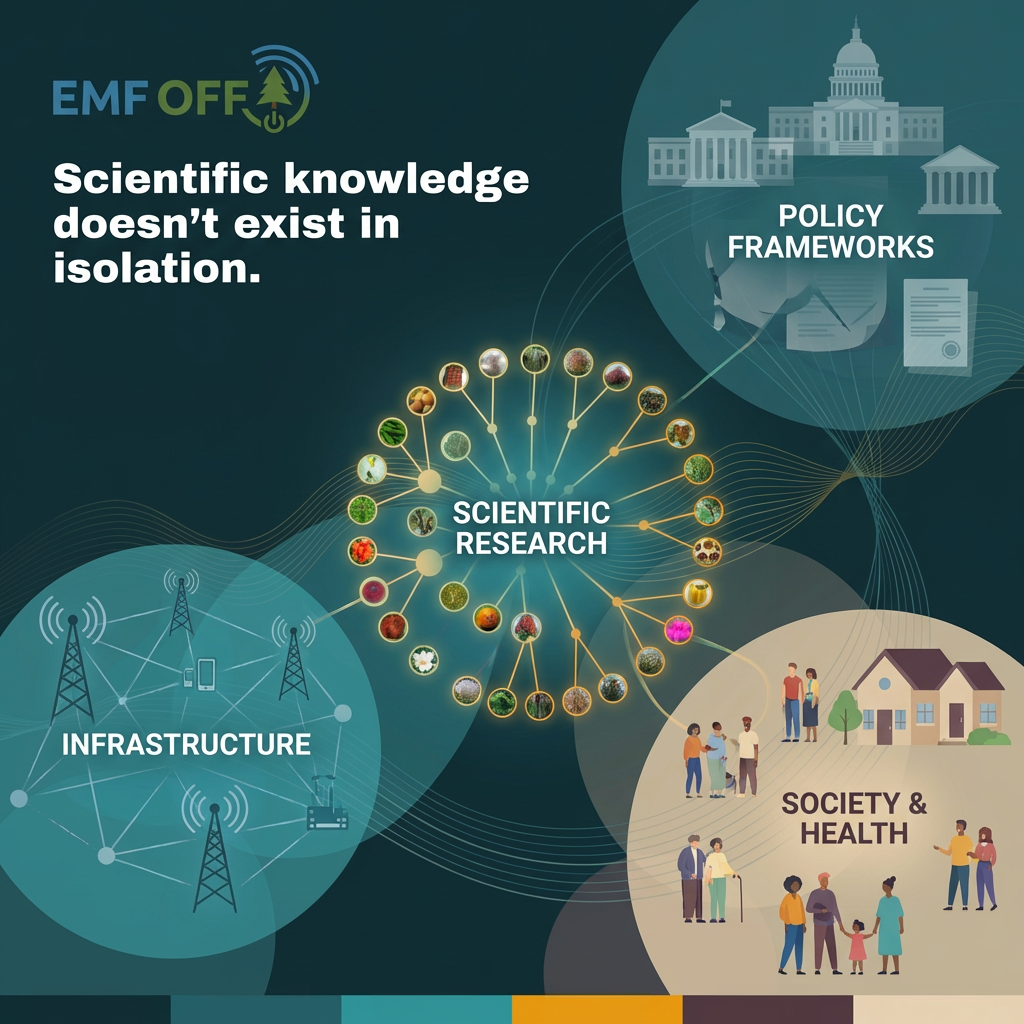
Scientific research does not occur in a vacuum.
It exists within networks of funding, regulation, infrastructure, and public health priorities.
Those surrounding systems influence which questions are asked — and which are considered settled.
Funding Directs Attention
Research agendas often follow available funding streams.
When funding prioritises certain mechanisms or endpoints, those areas accumulate data more quickly.
Over time, this can shape what appears most established — not necessarily because other questions lack merit, but because they receive less sustained investigation.
Standards Reflect Assumptions
Safety standards are built on specific biological assumptions.
If harm is defined primarily as tissue heating, studies will be designed to measure heating.
Findings outside that framework may be documented — yet carry less regulatory consequence.
A Model With a History
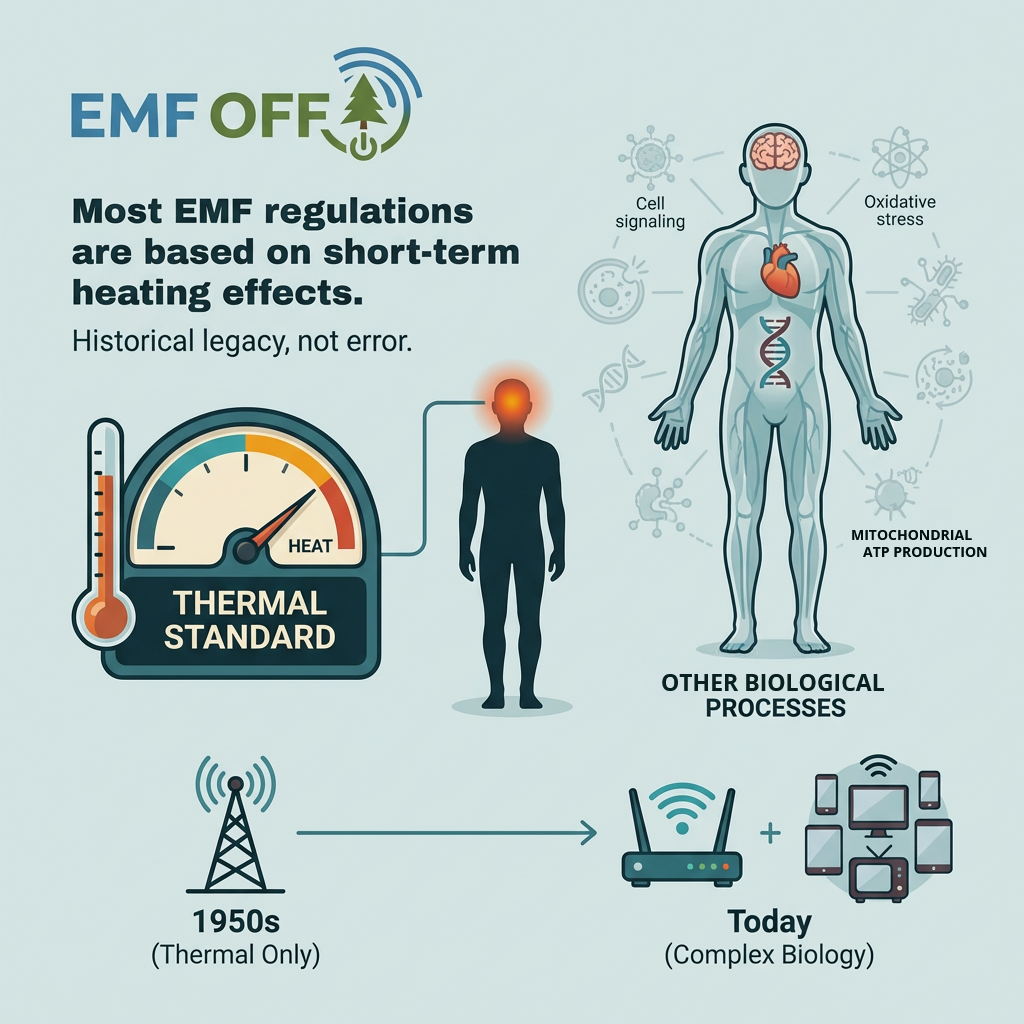
Current exposure limits were originally designed around short-term thermal effects.
This approach made sense given the scientific tools and knowledge available at the time.
As biological understanding evolves, frameworks do not always evolve at the same pace.
Complex Effects Are Harder to Capture
Subtle biological responses — oxidative stress, cellular signalling changes, mitochondrial shifts — are more difficult to measure than acute heating.
They may require longer time horizons, different endpoints, and more nuanced experimental design.
Complexity often slows consensus.
Absence Within a Model
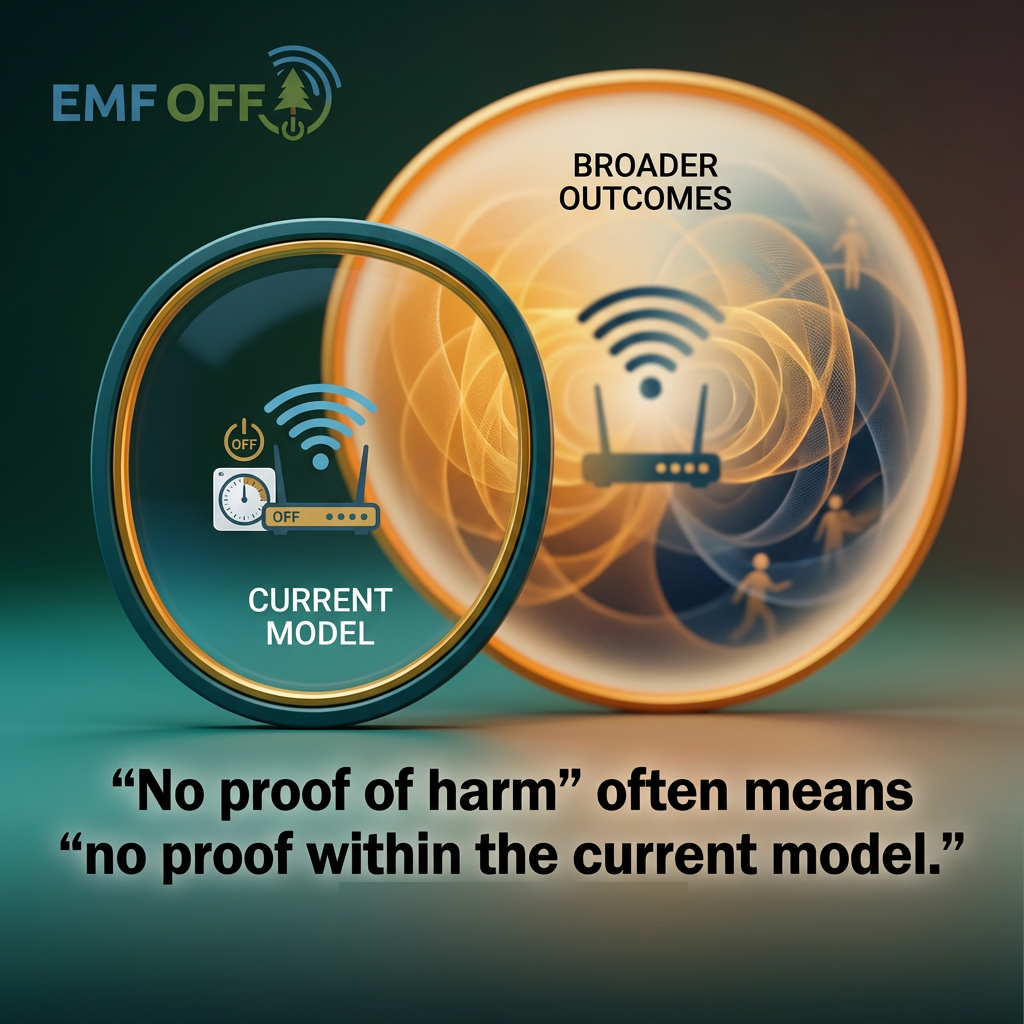
When authorities state “no proven harm,” this nearly always refers to harm as defined within the prevailing framework.
If the framework measures thermal injury, non-thermal findings may be considered inconclusive rather than irrelevant.
Definitions matter because they determine what counts - and what is excluded.
Institutional Inertia Is Predictable
Revising exposure standards would affect infrastructure, compliance requirements, and long-standing regulatory positions.
Large systems tend to resist shifts that introduce uncertainty or cost.
This resistance does not require malicious intent — only structural incentive alignment.
Historical Precedent
In other public health cases — tobacco, lead, asbestos — early biological signals preceded regulatory action by years or decades.
In each case, economic interests influenced how emerging data were interpreted and communicated.
Scientific debate and financial stakes often intersect.
When Clarity Is Slow
Regulation typically follows established consensus, not early warning signals.
During periods of uncertainty, individuals are left to interpret incomplete information.
Risk navigation becomes decentralised.
Prudence in the Gap
Choosing precaution does not require certainty of harm.
It reflects a judgment about uncertainty, vulnerability, and values.
Different individuals will draw that line differently — especially when children are involved.
Where this leads
Recognising structural influence does not, by itself, determine the magnitude of risk.
History shows that economic and regulatory inertia can delay response to emerging biological signals.
When uncertainty intersects with plausible mechanisms and vulnerable populations,
the question becomes practical: what level of precaution is reasonable?